This post is about emotional support for people suffering infertility — I hope you’ll read through to the end, but if you don’t, please please check out the Fertility Network UK #CryingShame fundraiser , to ensure every patient across the country going through fertility issues gets the individual support and advice Fertility Network UK offers.
Infertility sucks
Infertility isn’t just hard. It isn’t just sad. It isn’t just difficult. Please understand that infertility is deeply traumatic and utterly harrowing.
One study by Fertility Network UK found that that 90% of infertile couples reported feeling depressed, while 42% reported feeling suicidal.
A study looking specifically at the psychological impact of failed IVF found that 94% of the women surveyed had experienced symptoms of depression and anxiety, whilst 13% had experienced suicidal ideation.
In another study, 50% of women said that infertility was the most upsetting experience of their lives.
One study even found that levels of depression and anxiety in infertility patients were comparable with cancer patients.
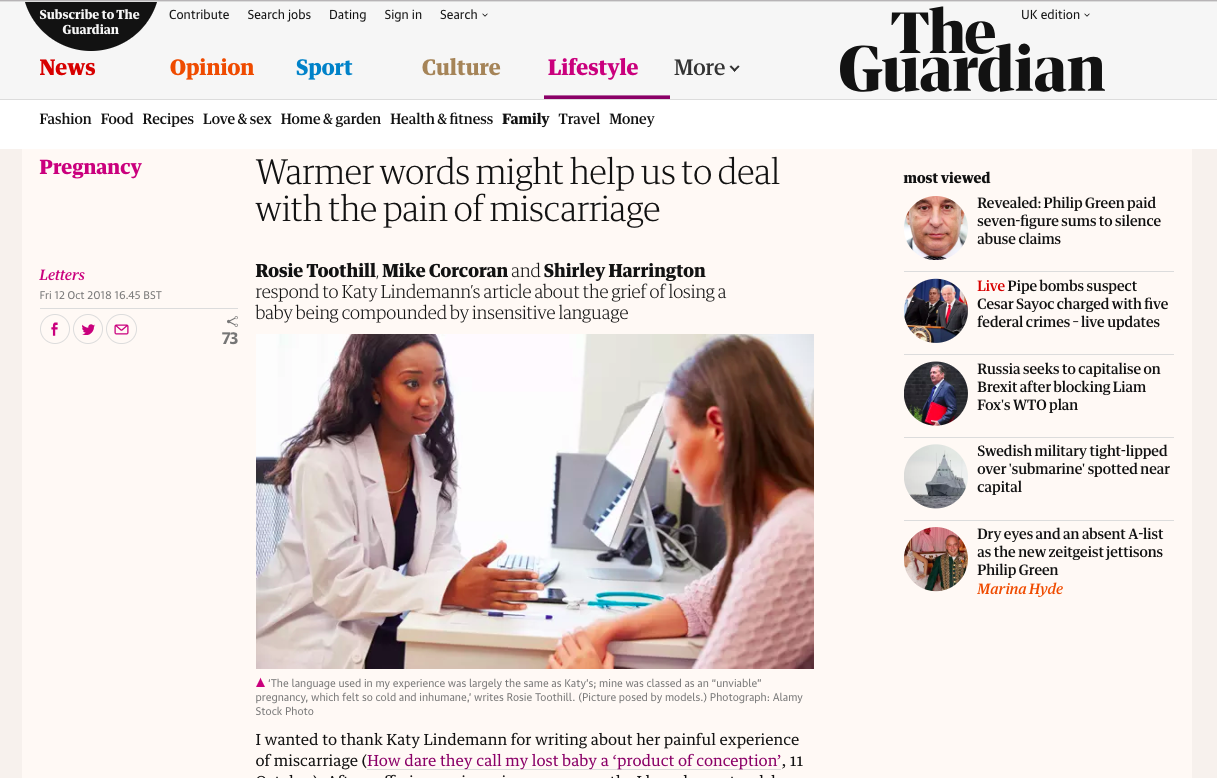
A recent study found 4 in 10 women experienced symptoms of post-traumatic stress disorder after a miscarriage. Other studies show the depression and anxiety experienced by many women after a miscarriage can continue for years.
In short, infertility and pregnancy loss are life-changing and life-defining.
I was lucky that during my fertility journey I experienced excellent patient support — which isn’t just about paying lip service to patient support by offering a token session of counselling. For me it’s about the everyday interactions — kindness from clinicians and clinic staff, being responsive to questions, and recognition that whilst we’re just one patient of many, for us this is one of the most important and challenging experiences of our life. Understanding from family and friends was key, and finding my tribe in support groups on and offline kept me sane.
So what does good support for someone going through infertility look like?
How to support patients
The HFEA have developed a new Code of Practice for clinics in the UK, which now has a dedicated section specifically for patient support: specifying clinics’ responsibilities not only to make counselling accessible, but to develop a patient support policy that codifies how the clinic will ensure all staffprovide “appropriate psychosocial support” before, during and after treatment.
Some suggestions of what I think ‘appropriate psychosocial support’ should look like:
Clear written information: given at the start of treatment to provide clear information about the proposed treatment to prepare patients about what to expect; detailing all emotional support available, and the importance of accessing it for patients’ mental health, and signposting relevant organisations and resources.
Defined follow-up protocols: for people who have successful and unsuccessful treatment, as well during the two-week wait.
Open-door access to fertility counselling and coaching: as both a support system to help patients cope, and a sounding board to help patients find ways to move forward with their goals.
Support groups: mixed, male, female and specific interest (e.g. LGBT parents, solo motherhood) — either in-clinic or clear signposting to those that already exist elsewhere (such as the excellent support groups and workshops by Fertility Network UK, and other organisations such as the Donor Conception Network
How to support family or friends suffering infertility
There’s no universally right or wrong answer: the ‘right’ thing will vary immensely from person to person — and indeed the same person on different days. However, I found that there are some general dos and don’ts that are pretty safe bets and will make an enormous difference to a friend or loved one suffering from:
Say ‘I’m sorry’ Give us a hug and say ‘I’m so sorry’.
Do not try to solve the problem There’s nothing you can say or do to fix this, so stop trying to do so.
Don’t tell us about miracle babies Please, please don’t offer advice or tell us about someone else’s miracle story — all you can do is bear witness to our pain. Just listen & acknowledge our distress Don’t feel you have to do anything other than listen.
Don’t tell us what to do or what to think or what to feel. Just listen to us, and allow us to be sad and angry at how unfair life is. Be there, let us know you care, that you’re there, and that you want to understand our feelings and needs. Acknowledge that it’s an unimaginably cruel situation and let us offload
Don’t diminish our suffering by telling us we’re being oversensitive, or that we should be over it by now. It’s OK for us to not be OK.
Try not to take it personally if we withdraw from social situations or distance ourselves from you. It’s not that we don’t care — we do. We’re just trying to protect ourselves from being hurt even more than we already are.
Don’t ignore it Recognise our devastation and ask us if we’d like to talk about it. Don’t be fooled that our smiles mean that everything’s fine. We might not want to talk about it — but just letting us know you’re thinking of us can go a long way.
Reassure us that you love us Don’t ever say that it’ll happen eventually — because you don’t know that it will (and it might not). Reassure us that you love us and will support us no matter what — that we are still loved and important, regardless of whether we become parents.

How you can make a difference
It’s a #CryingShame that people struggling to conceive experience depression and anxiety without adequate support. It’s a #CryingShame that there is also a severe lack of funding for patient support in fertility services.
Which is why Fertility Network UK have launched a 30 day fundraising appeal to ensure every patient across the country going through fertility issues gets the individual support and advice Fertility Network UK offers.
Fertility Network UK provide invaluable information and support for people going through an infertility journey, and they are a brilliant cause I’m proud to support.
Please, please give generously, and please, please share the campaign. So many people are suffering in silence — you probably know someone who’s suffering but who may not feel brave enough to speak out about what they’re going through. Fertility Network UK supports thousands of people who are living this in the shadows, and by supporting their fundraising and their initiatives, you will be making a difference to so, so many people.
Maybe even someone you know and love.
[ Some of this content was previously published in pieces I wrote for Fertility Fest and for Metro’s Fertility Month]